What Do Hospitalized Patients Say Would Be Worse Than Death?

Survey says…
In caring for hospitalized patients with serious illnesses, and in evaluating interventions designed to help them, clinicians and researchers often focus on death as the primary outcome to be avoided. We tend to pay less attention to avoiding other outcomes that may be equally or more unacceptable to some patients.
Between July 2015 and March 2016, Anna Buehler, Scott Halpern, and I asked 180 patients with serious illnesses who were hospitalized at the Hospital of the University of Pennsylvania to rate a series of single-dimension health states on a 5 point Likert scale with options of worse than death, neither better nor worse than death, a little bit better than death, somewhat better than death, or much better than death. The results, which were recently published in a research letter to JAMA Internal Medicine, are shown in the table below.
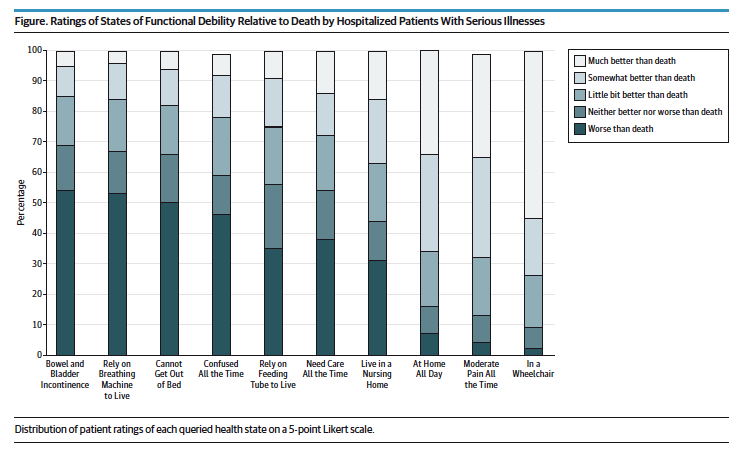
The responses varied widely, but a large proportion of patients said that they would consider certain states of physical and cognitive debility – including bowel and bladder incontinence, relying on a breathing machine to live, being bed bound and being confused all the time – to be equal to or worse than death. Our findings are consistent with previous studies of healthy patients and non-hospitalized patients with serious illness.
Can we take these results literally? Are we to believe, for example, that a majority of patients with serious illnesses would rather die than go on living if they were to develop incontinence? There are reasons to be cautious in how we interpret the responses patients gave. First, we intentionally asked about single dimension states of debility, and patients undoubtedly had varying impressions in their minds of what such states might involve. Incontinence, for example, can be associated with more global deterioration of physical and cognitive function, but it can also be an isolated impairment. There is a cognitive bias known as a focusing effect, where people overemphasize one feature or attribute of a decision at the expense of others that may lead them to a different conclusion. The answers our cohort gave likely were influenced to a certain extent by focusing effects. Also, most of the patients we talked to were not actually currently experiencing the health states we asked them to consider. We know that people have some difficulty predicting how they might feel if they find themselves in a particular situation in the future (known as affective forecasting). When they are actually faced with a situation, people may adapt to things they once imagined they would find intolerable.
Although we should be cautious in interpreting our results literally, we should nevertheless pay attention to them. Even considering the limitations of the data, the distribution of responses strongly suggests that many people who have already been diagnosed with a serious illness would consider certain states of debility and loss of control to be intolerable. With that in mind, we need to consider more carefully the impact of our medical interventions in patients who have potentially life-limiting illnesses, particularly those associated with progressive debility.
It is easy to focus on avoiding mortality, both because it is an outcome that we know most people wish to avoid and because it is easily measurable. States worse than death are much more subjective and are therefore harder to define and quantify. But whether we are making clinical decisions for patients with serious illnesses, designing research studies assessing the impact of various interventions, or developing quality metrics to evaluate how well we are caring for people, we need to pay more attention to avoiding suboptimal outcomes other than death.
This blog post originally appeared on LDI Health Policy$ense.